Information on the development of the functionality of MIS and RMIS in terms of resuscitation and anesthesiology
Problems in the automation of resuscitation and intensive care for the end customer
- Manual entry of a large number of parameters by employees of the Ministry of Defense, to the detriment of time for decision-making and work with patients;
- High probability of errors in manual data entry;
- High cost of specialized solutions and integration of MIS with these solutions.
For MIS and RMIS developers
- The need for integration with specialized systems (if they are implemented by the Client) with a large amount of information transferred between systems;
- Lack of drivers and middleware solutions for connecting the appropriate equipment as a class in the Russian market;
- Lack of open access documentation for equipment and closed protocols for the interaction of information systems with equipment;
- Equipment manufacturers do not provide information support to developers from the Russian Federation;
- Shortage in the labor market of developers with low-level programming skills;
- Delaying the budgets of Customers for the implementation of specialized solutions.
Documentation and functionality of MIS in anesthesiology and intensive care
Surgical operations and intensive care are among the most difficult and critical stages of patient treatment, requiring maximum concentration, attention, speed and quality of decision-making from medical personnel.
These stages of treatment are accompanied by a large set of medical documentation, including such voluminous documents as an anesthesia course map and an intensive care map. These documents can be seen in Figures 1 and 2.
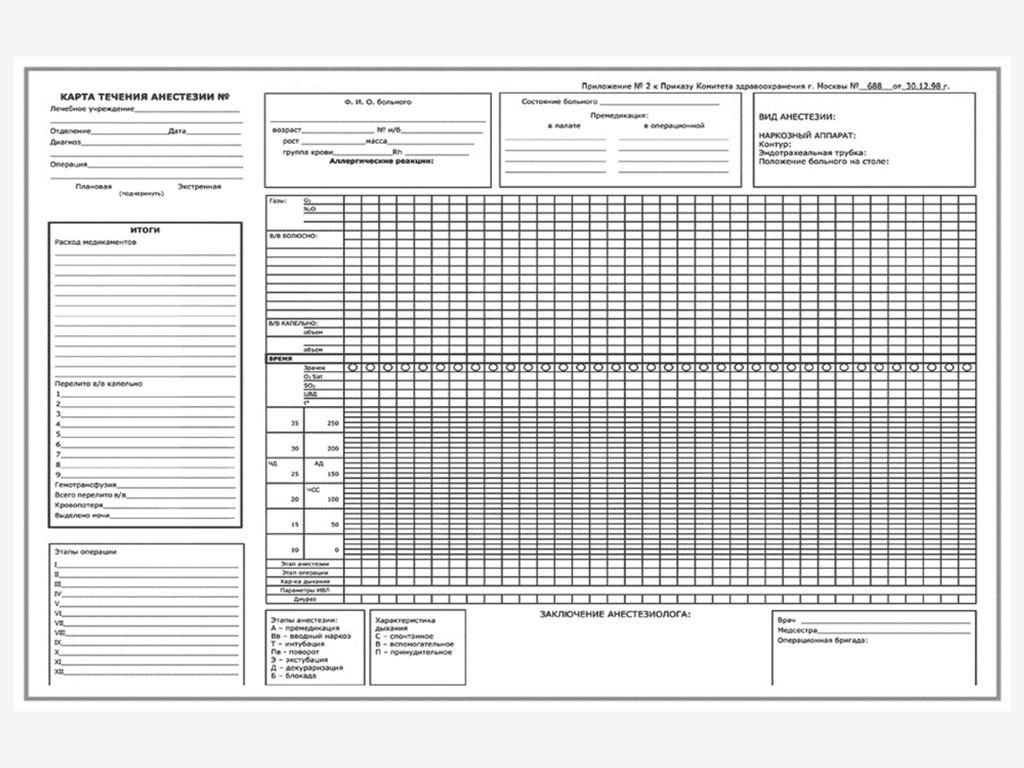
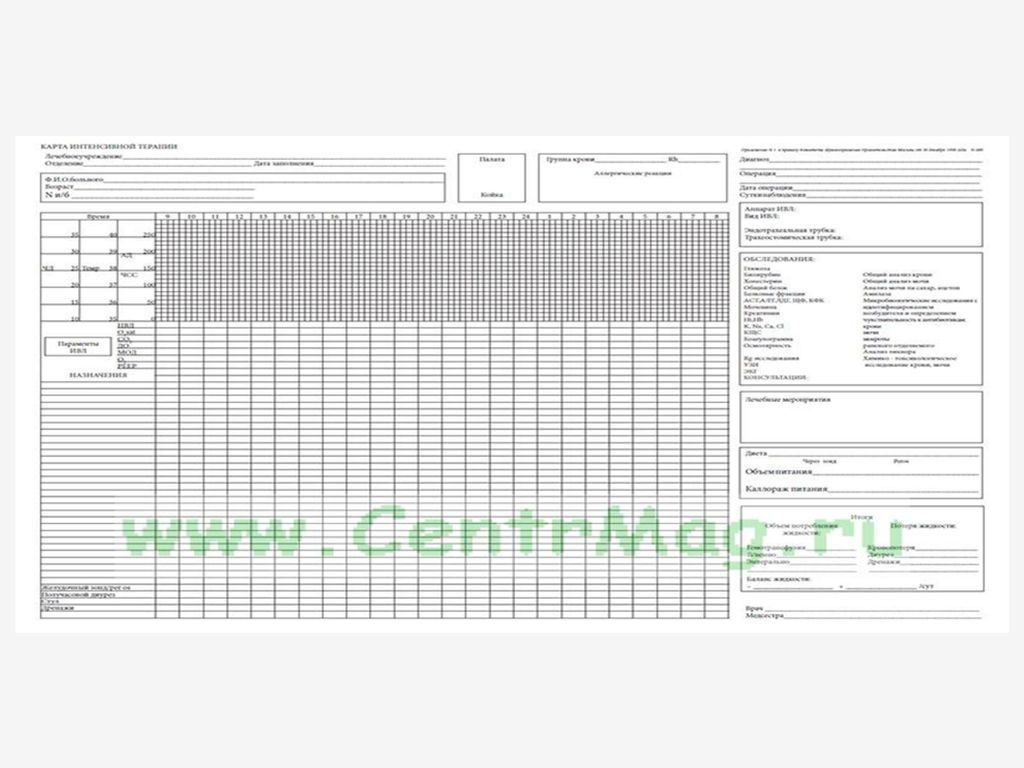
The cards themselves contain the following amount of information:
- Medical appointments;
- Medical manipulations and stages of the operation;
- Fluid balance;
- Results of laboratory researches;
- Results of instrumental studies;
- Indicators of the patient's condition.
In addition to the cards themselves, such indicators are also used in other medical records generated at these stages of treatment, which makes the automatic transfer of data from equipment and the provision of a single entry at the indicated stages a necessity, designed to reduce the time spent by medical personnel on record keeping and their release to work. with patients and decision making.
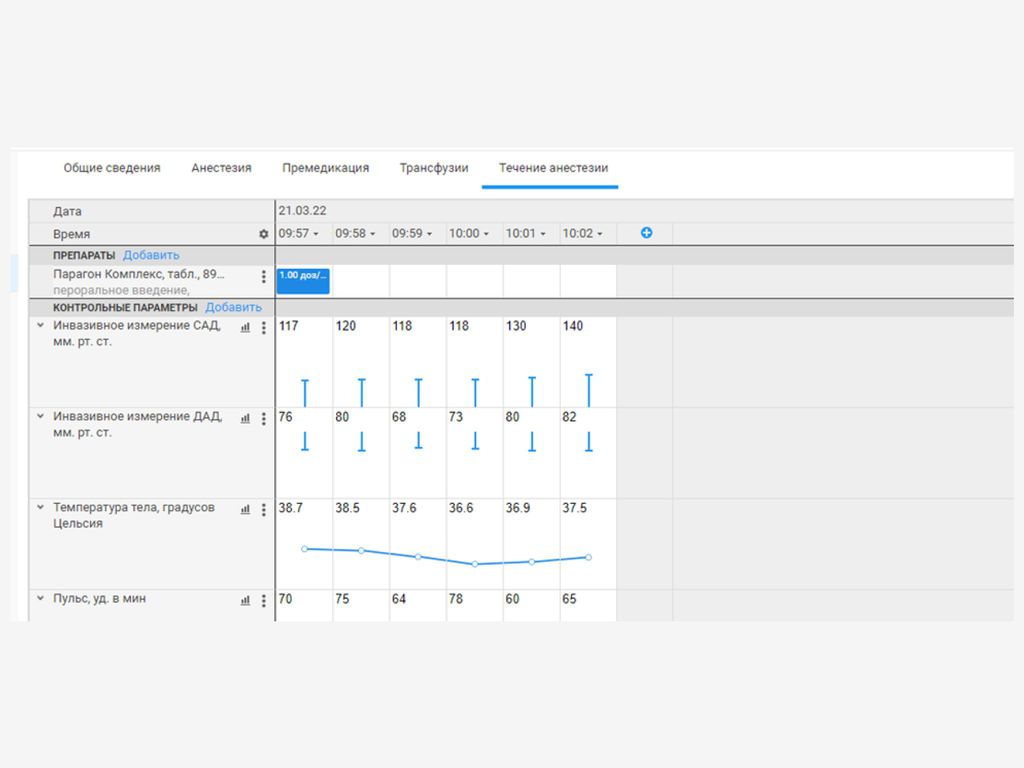
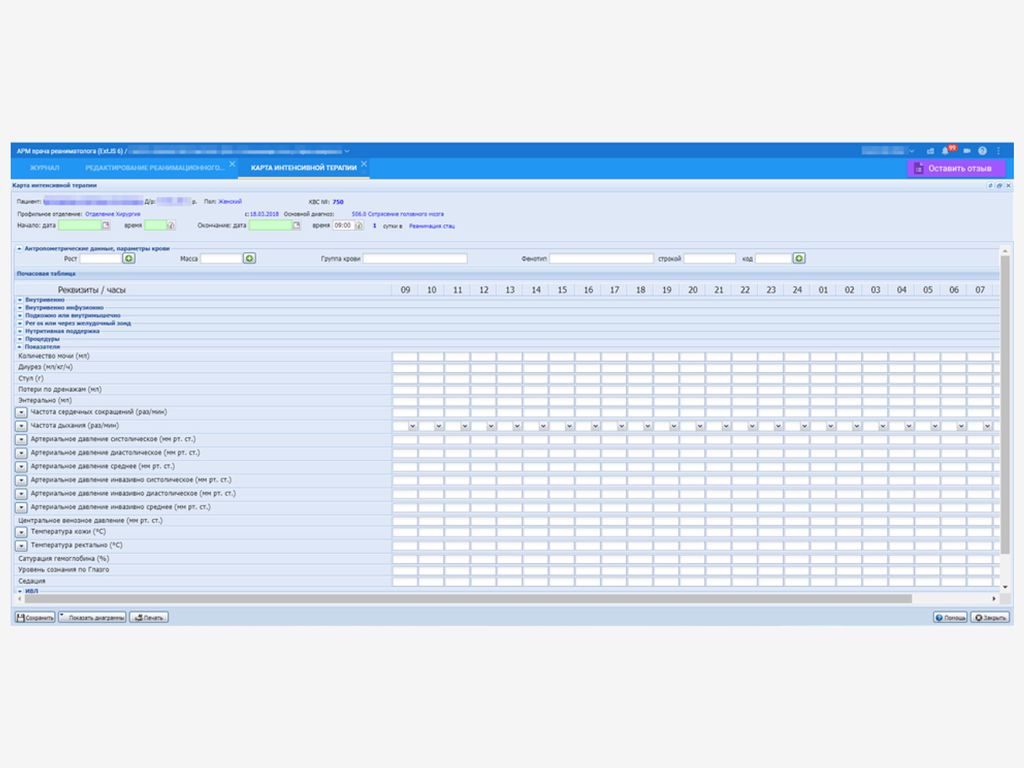
At the moment, most medical information systems (MIS and RMIS) in the Russian Federation to some extent implement the maintenance of cards in electronic form, for example, as shown in the following figures:
In a number of medical institutions, where, within the framework of the HIS or separately, but integrated with the HIS, there are laboratory information systems and automation systems for instrumental studies, the results of laboratory and instrumental studies can be entered into the cards automatically, also significantly reducing the burden on medical personnel and reducing the likelihood of manual data entry errors.
Unfortunately, it is not possible to completely eliminate the manual entry of data on prescriptions and manipulations, but HIS allows for various cases of operations and intensive care, according to methodological recommendations, to form and use pre-prepared templates, which also reduces the burden on medical personnel in terms of documentation .
However, there is a significant block of indicators of the patient's condition, which is still entered manually in most medical organizations of the Russian Federation. This block, depending on the complexity of the operation, the patient being on a ventilator and other conditions, can contain from 5 to about 25 parameters (in Figure 4, you can see 12 indicators without taking into account the ventilator). At the same time, for maps of the course of anesthesia, such a data set may require fixing every few minutes, and for intensive care maps - once an hour, but up to 8-10 patients can be under the supervision of one guard sister and one resuscitator at the same time. Entering this amount of information manually is time-consuming and increases the likelihood of errors that can further affect the quality of decisions made.
The identified problems can be solved by connecting resuscitation and anesthetic equipment to information systems (to MIS directly or through specialized software).
Also, if the functionality of the "hospital employee pager" is available, warnings about the deviation of the patient's condition indicators can be sent to the mobile application directly from the devices if a driver is available.
Connected equipment in anesthesiology and intensive care
Below are examples of indicators that can be obtained automatically in information systems when the following equipment is connected to them:
- Bedside monitor. It measures indicators such as:
- Heart rate;
- Arterial pressure systolic;
- Arterial pressure diastolic;
- Arterial pressure is average;
- Breathing rate;
- Saturation of hemoglobin;
- Central venous pressure;
- Temperature.
- Artificial lung ventilation apparatus or anesthetic-respiratory apparatus. Measure indicators such as:
- Oxygen concentration;
- Breathing rate;
- Respiratory volume;
- Minute volume of breath;
- Pressure at the end of exhalation;
- Peak inspiratory pressure;
- Mean airway pressure.
Specialized information systems available in the Russian Federation
In the Russian Federation, the most well-known projects are the implementation of specialized solutions based on foreign ICCA software from Philips.
The cost of implementing such solutions is much higher than the cost of implementing LIS or PACS. The estimated cost of implementing ICCA Philips is 900,000 rubles/bed.
The spread of such systems is significantly hindered by the need for deep and voluminous (compared to LIS and PACS) integration, since it is necessary to ensure not only the transfer of referrals and the receipt of results from the corresponding equipment, but also the integration of a pharmacy, a warehouse, additional directories and organize the exchange of other information about the patient and his treatment.
In world practice, developers of medical information systems actively use middleware that specializes in providing the ability to connect a significant range of such equipment directly to HIS using a single interaction protocol. Basically, these are products developed in the USA.